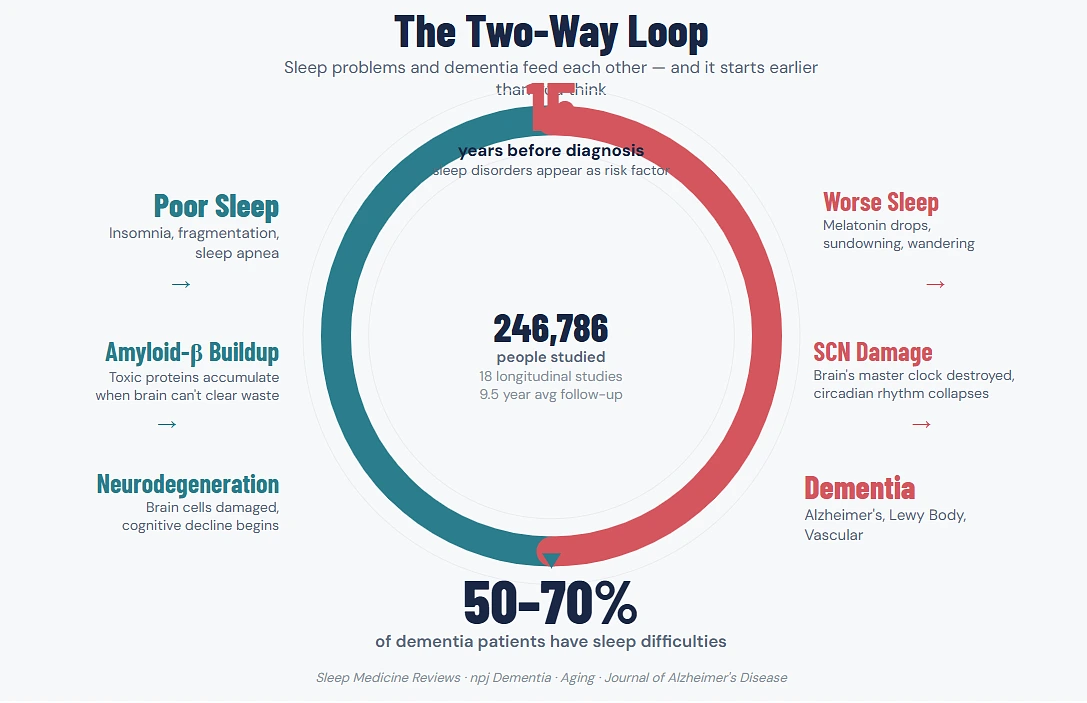
Between 50-70 percent of individuals diagnosed with dementia experience difficulties in sleeping and those figures were provided by clinical research published in the journal Aging, not by a wellness blog. Juxtapose it with the general older population where sleep issues are prevalent but nowhere close to such levels, and it becomes obvious that this is not old people not sleeping well. Something unique occurs in the dementia brain that destroys the normal sleeping ability and it begins earlier than the families anticipate.
The hard thing about taking care of someone with dementia is that the sleep issues do not come on a silver platter. They intersect, they change week to week and they impact the well-being of the caregiver nearly as much as they impact the patient. When a wandering person roams the hallway at 3am, they do not only deprive themselves of sleep, but everyone who was sleeping was also robbed of their sleep.
It Goes Both Ways — And That’s What Makes It Complicated
Most people assume sleep problems show up after a dementia diagnosis. That’s partly true, but it’s only half the picture.
A meta-analysis published in Sleep Medicine Reviews analyzed 18 longitudinal studies covering 246,786 people over an average follow-up of nearly 9.5 years. People with sleep disturbances had a measurably higher risk of developing all-cause dementia, Alzheimer’s disease, and vascular dementia compared to people without sleep problems. A separate study published in npj Dementia using over one million electronic health records from Wales and Finland found that sleep disorders showed up as a risk factor up to 15 years before dementia was clinically diagnosed (“Sleep disturbances as risk factors for neurodegeneration later in life” — npj Dementia, 2025).
Fifteen years. That’s not a coincidence — that’s a signal.
So the relationship runs in both directions. Dementia damages the parts of the brain that regulate sleep, which makes existing sleep worse. But poor sleep also appears to accelerate the biological processes that lead to dementia in the first place, including amyloid-beta buildup. A finding published in the Journal of Alzheimer’s Disease showed that cerebrospinal fluid amyloid-β levels were increased in patients with insomnia. Amyloid-beta is one of the proteins that accumulates in Alzheimer’s disease.
In plain terms: bad sleep doesn’t just happen because of dementia. Bad sleep might be helping dementia get started.
Not All Dementia Wrecks Sleep the Same Way
This part matters because families often don’t know that the type of dementia their loved one has directly shapes what kind of sleep problems to expect. Knowing the pattern helps caregivers prepare instead of reacting in the dark at 2am.
Alzheimer’s Disease
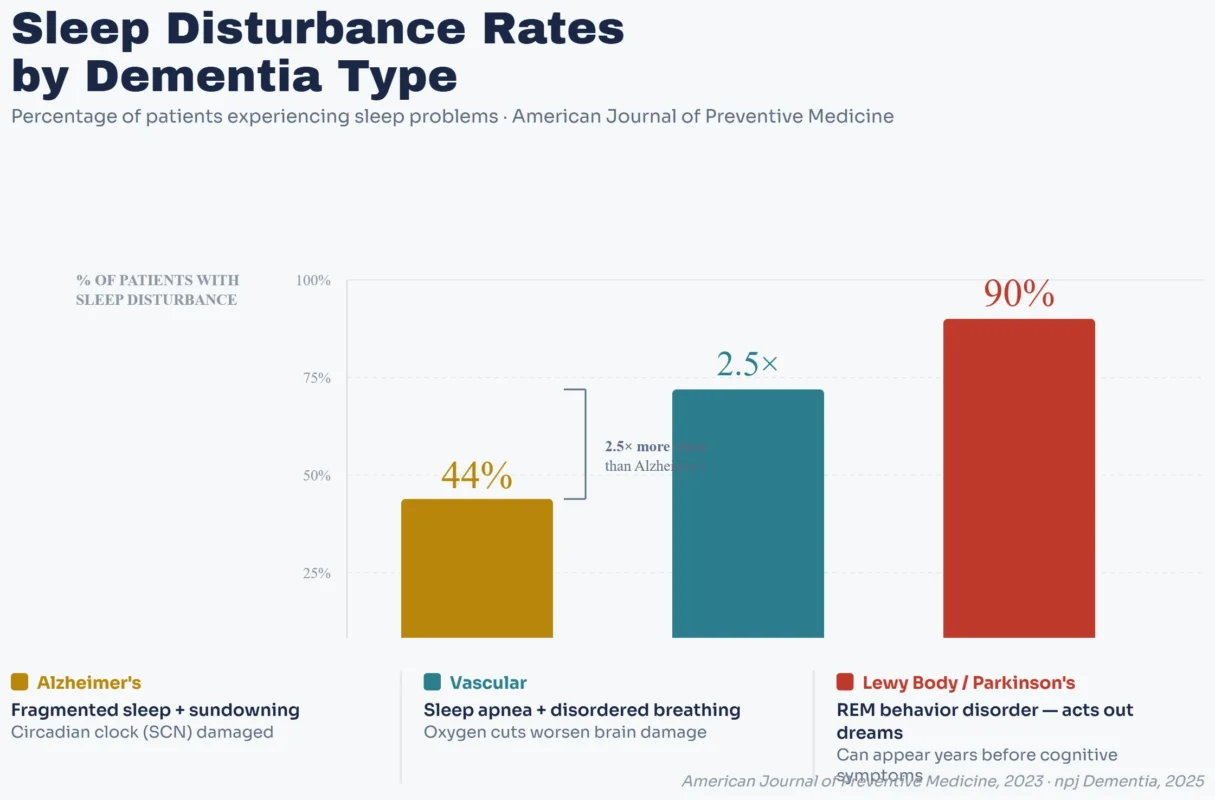
According to the figures reported in the American Journal of Preventive Medicine, up to 44% of Alzheimer patients suffer sleep disorders. Fragmented nighttime sleep (waking up several times and being unable to fall asleep again) and excessive daytime sleepiness (the individual nodding off and then being unable to sleep at night) are the most frequent ones. Because the suprachiasmatic nucleus, the small part of the brain that operates the circadian clock, has been damaged by Alzheimer, the circadian rhythm, the internal clock that tells you when to be awake and when to sleep, begins to divide.
Then there’s sundowning. Assuming you have ever been around someone with moderate, or advanced, Alzheimer’s, you have a fair idea of what this is, even though you may have never heard the term. In the late afternoon, or evening, the individual becomes more and more disoriented, agitated, restless, occasionally aggressive. It usually reaches its highest point at sunset – thus the name – and may render the interval between 4pm and bedtime the most difficult of the day to all the members of the house.
Lewy Body Dementia and Parkinson’s Disease Dementia
This is where sleep problems get genuinely alarming. Up to 90% of people with Lewy body dementia or Parkinson’s disease dementia have sleep disturbances according to the same American Journal of Preventive Medicine data.
The hallmark issue is REM sleep behavior disorder, and it deserves a clear explanation because it’s unlike anything most people associate with “sleep problems.” During normal REM sleep, the body is essentially paralyzed — your brain is dreaming but your muscles are switched off so you don’t physically act out what you’re experiencing. In REM sleep behavior disorder, that paralysis doesn’t happen. The person physically acts out their dreams. They punch, kick, shout, fall out of bed, sometimes injure themselves or their sleeping partner.
What makes this especially important is that REM sleep behavior disorder frequently appears years before any cognitive symptoms show up. It can be one of the earliest detectable signs that Lewy body or Parkinson’s pathology is developing in the brain. The majority of people diagnosed with REM sleep behavior disorder eventually develop one of these conditions, per research cited in npj Dementia.
Vascular Dementia
According to the American Journal of Preventive Medicine, patients with vascular dementia experience sleep disturbance 2.5 times more often than in patients with Alzheimer or frontotemporal dementia. Here especially is sleep-disordered breathing, which encompasses obstructive sleep apnea. This relationship is biologically plausible in that vascular dementia entails the destruction of blood vessels in the brain, and sleep apnea periodically cuts the oxygen supply to the brain at night, furthering the vascular destruction already present.
What Caregivers Actually Deal With at Night?
Research papers describe sleep disturbances in clinical terms. Caregivers describe them differently.
A once-a-night sleeper now wakes 4 or 5 times and attempts to get out of the house. They believe that it is morning, when it is midnight. They get dressed, seek keys to the car, attempt to make a breakfast at 3am. Or they are sitting on the edge of the bed crying and not knowing why. Or they get aggressive as someone attempts to take them back to bed since in their state of confusion, the caregiver appears like a stranger.
An Italian multicentric study conducted in PubMed found that more than 60% of MCI and dementia patients reported 1 or more sleep disturbances and that the issues were virtually always co-morbid ( Italy (PubMed) Prevalence of sleep disturbances in mild cognitive impairment and dementing disorders” — PubMed, 2012). It is not often only insomnia or only daytime sleepiness. It’s a starting to feed on itself thing, bad nights, make you have exhausted days, exhausted days, make you have irregular napping, irregular napping, make the next night worse.
And here’s the part that doesn’t make it into enough conversations: sleep disturbance is one of the leading reasons families make the decision to move a loved one into a care facility. Not because they stop loving them. Because the caregiver physically cannot sustain months or years of broken sleep while providing round-the-clock supervision during the day. Research published in Aging confirmed that these disturbances contribute to increased caregiver stress, higher rates of institutionalization, and accelerated cognitive decline in the patient.
The caregiver’s own sleep deprivation becomes its own medical problem. It affects their immune system, their mental health, their ability to make decisions about the person they’re caring for. Ignoring it isn’t sustainable and it’s not noble — it’s a path toward two people being unwell instead of one.
When to seek professional help?
It is important to consult a mental health professional specialized in insomnia treatment, if a dementia patient is experiencing these problems, such as:
- Sleep issues persist for more than 2 weeks
- Loud snoring and intermittent breathing during sleep
- Physical pain
- Constantly fall asleep during the day
- Concerns such as dizziness and an increased risk of falls at night
- Impact on day-to-day activities
- Impact on the relationship
A mental health professional, such as board certified neuropsychiatrist, can understand the brain changes associated with dementia, as well as the sleep problems that come with it. They help with:
- Prescribing melatonin supplements to establish a proper sleep cycle
- Treating medical conditions that alter sleep
- Changes to medications currently being taken that interfere with sleep
- Sleep studies to diagnose sleep disorders like sleep apnea
What’s Actually Going Wrong in the Brain
Without getting buried in neuroscience, a few biological things are happening that explain why sleep falls apart in dementia.
The suprachiasmatic nucleus — a cluster of about 20,000 neurons in the hypothalamus — is the brain’s master clock. It receives light signals from the eyes and uses them to regulate the circadian rhythm, telling the body when to produce melatonin (which promotes sleep) and when to suppress it (which promotes wakefulness). In Alzheimer’s disease, this region sustains direct damage as the disease progresses, which is why the day-night cycle starts losing its grip on the patient’s behavior.
Melatonin production drops. Older adults naturally produce less melatonin than younger people, but in dementia patients the decline is more pronounced. This contributes to difficulty falling asleep and to the general blurring of daytime and nighttime alertness levels.
There’s also a medication problem that doesn’t get discussed openly enough. Cholinesterase inhibitors like donepezil, which are commonly prescribed to manage cognitive symptoms in Alzheimer’s, can cause vivid dreams, nightmares, and insomnia as side effects. The very medication meant to help cognition can make sleep worse. And on the other end, benzodiazepines — sometimes prescribed to help patients sleep — have been linked to increased dementia risk in a review and meta-analysis cited by npj Dementia. So the medication landscape for sleep in dementia patients is genuinely difficult to get right, because several common options either cause sleep problems or potentially accelerate cognitive decline.
What Can Actually Be Done
Start Without Medication
A PMC paper focused specifically on nursing interventions for dementia patients with sleep disturbances was clear on this point: non-pharmacological measures should come first (“Sleep disturbances in dementia: What they are and what to do” — PMC).
- Bright light exposure during the day — helps recalibrate the circadian rhythm. Natural sunlight is best, but therapeutic light boxes work when outdoor time isn’t practical. The goal is telling the damaged internal clock that daytime is daytime.
- Structured physical activity — even moderate exercise like walking reduces daytime sleepiness and improves nighttime sleep consolidation. Timing matters. Activity in the morning or early afternoon is better than late in the day.
- Consistent sleep schedule — same bedtime, same wake time, even on bad nights. The routine becomes an external structure replacing the internal clock that’s failing.
- Reduce nighttime noise and light — dementia patients in care facilities are especially vulnerable to environmental disruptions. Hallway lights, staff conversations, other residents — all of it fragments already fragile sleep.
- Limit daytime napping — difficult in practice because the person is genuinely tired, but long or frequent daytime naps directly undermine nighttime sleep. Short naps (under 30 minutes) before early afternoon are a reasonable compromise.
When Medication Is Considered
If non-pharmacological approaches don’t get you far enough, then there are some that are less risky than others. Melatonin supplementation proved to have some benefit in some studies and has a relatively low profile of side effects. Trazodone, a sedating antidepressant, is sometimes used off-label for sleep for dementia patients and has a better safety profile than benzodiazepines.
What should generally be avoided: benzodiazepines (associated with increased risk of dementia, falls and cognitive worsening), anticholinergic sleep aids such as diphenhydramine (directly counteracts the effects that cholinesterase inhibitors are attempting to facilitate), and sedative-hypnotics (increases risk of confusion and falls in elderly patients).
Any medication choice for a dementia patient’s sleeping needs to be made with the prescribing physician, considering the nature of the dementia, the medications being taken now, fall risk, and what’s actually disturbing the sleep in the first place.
Don’t Forget the Caregiver
This isn’t an afterthought — it’s a clinical priority. Caregivers who burn out from chronic sleep deprivation can’t provide safe care. Respite care, shared caregiving schedules with other family members, and honest conversations with healthcare providers about the caregiver’s own sleep health all matter. There’s no version of this where the caregiver running on three hours of sleep for six months straight produces good outcomes for anyone involved.
When Sleep Problems Show Up Before the Diagnosis
For families faced with loved one who is already living with dementia, the sleep info above is immediately practical. But for folks in their 50s and 60s to start noticing chronic sleep problems developing – persistent insomnia, a bed partner reporting that they’re acting out dreams violently, increasing daytime sleepiness despite adequate nighttime hours – the research has a different kind of weight.
Obstructive sleep apnea is observed in approximately 50% of people with Alzheimer’s, and sleep disorders were predictive of neurodegenerative disease risk up to 15 years ahead of time, in one study published in npj Dementia that found that these risk factors were independent of genetic risk. That means attacking sleep apnea and chronic insomnia very aggressively now — with CPAP for sleep apnea, cognitive behavioral therapy for insomnia, better sleep hygiene — isn’t just about feeling rested tomorrow. It may be about protecting the brain 10, 15 years down the line.
That’s not a guarantee. But it’s enough of a signal that ignoring persistent sleep problems after age 50 seems like a risk most people wouldn’t want to take if they understood what the data was showing.
References
- “Sleep deprivation in dementia comorbidities” — Aging, 2024 – https://www.aging-us.com/article/206157/text
- “Sleep disturbances increase the risk of dementia: A systematic review and meta-analysis” — Sleep Medicine Reviews, PubMed, 2017 – https://pubmed.ncbi.nlm.nih.gov/28890168/
- “Sleep disturbances as risk factors for neurodegeneration later in life” — npj Dementia, Nature, 2025 – https://www.nature.com/articles/s44400-025-00008-0
- “Sleep Disturbances and Dementia Risk in Older Adults: Findings From 10 Years of National U.S. Prospective Data” — American Journal of Preventive Medicine, 2023 – https://www.ajpmonline.org/article/S0749-3797(23)00009-0/fulltext
- “Prevalence of sleep disturbances in mild cognitive impairment and dementing disorders: a multicenter Italian clinical cross-sectional study on 431 patients” — PubMed, 2012 – https://pubmed.ncbi.nlm.nih.gov/22415141/
- “Sleep disturbances in dementia: What they are and what to do” — PMC – https://pmc.ncbi.nlm.nih.gov/articles/PMC3062259/
- “Sleep Disorders & Dementia” — Practical Neurology – https://practicalneurology.com/diseases-diagnoses/alzheimer-disease-dementias/sleep-disorders-dementia/31539/
- “Prevalence of sleep disturbances in people with dementia living in the community” — ScienceDirect, 2022 – https://www.sciencedirect.com/science/article/pii/S1568163722002240